
The Advance Beneficiary Notice of Non-Coverage (ABN), is a notice given to Medicare beneficiaries to convey that Medicare is not likely to cover the service provided, or it is issued by providers in situations where Medicare payment is expected to be denied.
It is important to note that physicians’ offices must complete the ABN and deliver the notice to beneficiaries or their representative for review, and any questions raised during that review must be answered before it is signed. This ensures that the patient or their representative has time to consider the options and make an informed choice.
Once all the blanks are completed and the form is signed, the physician’s office then gives a copy to the beneficiary or representative. CMS mandates that the provider retain a copy of the ABN on file.
All of this is required before providing the items or services that are the subject of the ABN. If these procedures are not followed or the form is filled out incorrectly, the ABN is considered invalid. In certain cases, an invalid ABN could require repayment by the provider for all services rendered, as well as sanctions.
To quote Medicare, “Medicare will hold any provider who either failed to give notice when required, or gave defective notice, financially liable. Additionally, when authorized by law and regulations, sanctions under the Conditions of Participation (COP) may be imposed. A provider who gave defective notice may not claim that she/he did not know or could not reasonably have been expected to know that Medicare would not make payment as the issuance of the notice (albeit defective) is clear evidence of knowledge.”
As a chiropractic compliance consultant, I’m always asked about filling out an ABN for non-covered services (i.e. therapies, exams, and x-rays). The ABN is only required when you feel a service will be denied, and for chiropractic physicians, the adjustment is the only covered service.
If you wish to issue an ABN as a courtesy to the beneficiary, advising them of any financial liability for services that Medicare never covers (anything that’s not an adjustment), you can. This is called a voluntary ABN and this is considered non-valid by Medicare. If an office chooses to issue a voluntary notice, the beneficiary doesn’t need to choose an option box and is not required to sign the notice.
A better way to do this would be to design a statement form that tells the patient that Medicare only covers the adjustment and that the patient will be financially responsible for non-covered services provided as part of your treatment.
The ABN is approved by the Executive Office of Management and Budget (OMB) under the Paperwork Reduction Act of 1995 and is subject to re-approval every 3 years.
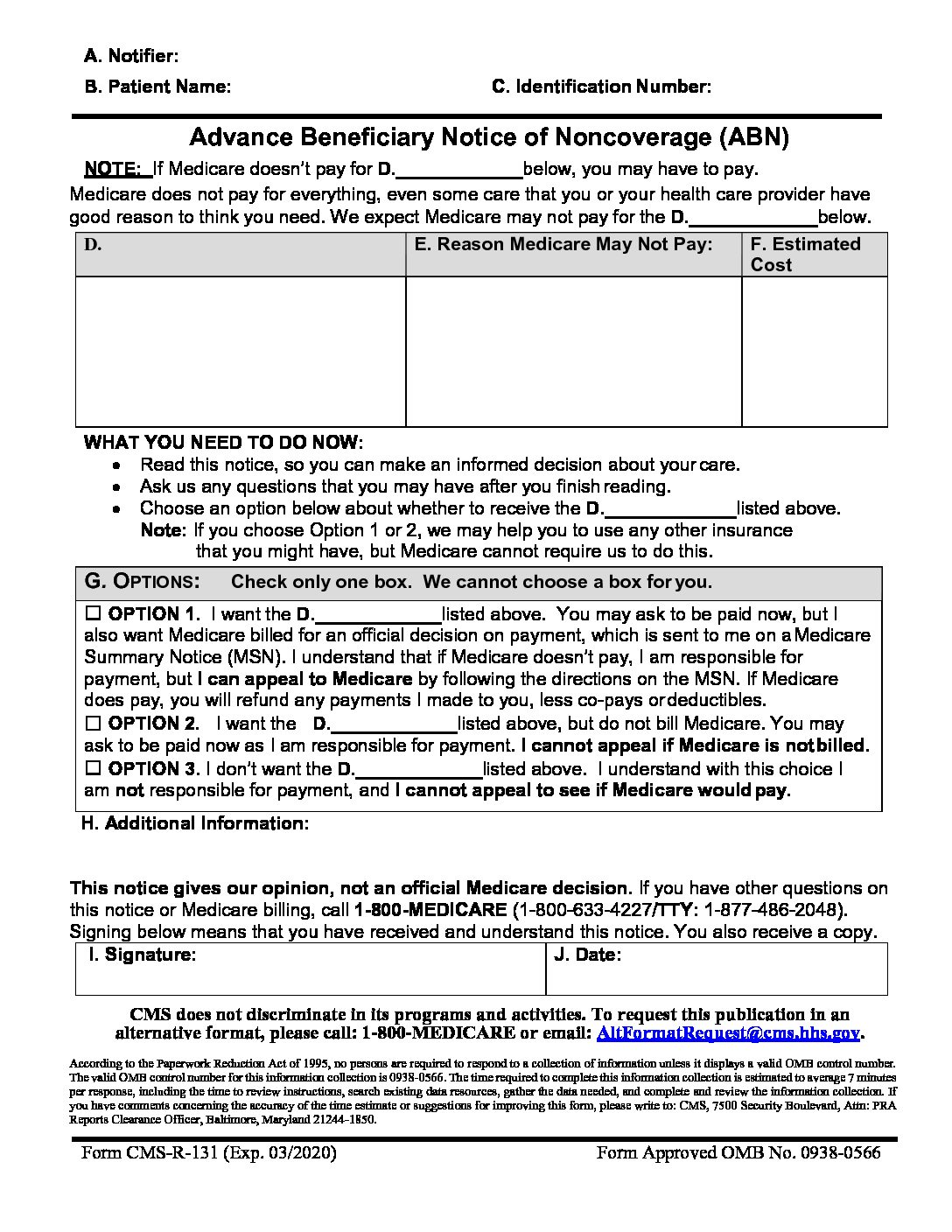
With that said, the form has been revised to include language informing beneficiaries of their rights to CMS non-discrimination practices and how to request the ABN in an alternative format if needed.
Providers are expected to exclusively use the current version of the ABN, and even though there are no changes to the form itself, providers must pay attention to the OMB approval date on the notice and obtain the current version. The date of mandatory use of the new ABN starts with claims made on or after 06/21/2017.
The new ABN form may be downloaded using the following links:
English version:
https://complianceandauditingservices.com/wp-content/uploads/2017/06/ABNEnglish2020v508.pdf
Spanish Version:
https://complianceandauditingservices.com/wp-content/uploads/2017/06/ABNSpanish2020-v508.pdf
You should be able to click on the links. If you have problems with the link just copy and paste it into the browser, then click enter.
Hopefully, this Compliance & Auditing Services notice will give you time to switch to the newly approved notices.
If you have any questions or need help, don’t hesitate contacting Compliance & Auditing Services.
All the Best,
Dr. John Davenport
Chief Compliance Officer
Compliance & Auditing Services

 Starting with the reporting year 2017, the current fee for service method of reimbursing physicians is going to evolve into a value-based methodology. Ignoring these changes can have a profound effect on your cash flow and profitability.
Starting with the reporting year 2017, the current fee for service method of reimbursing physicians is going to evolve into a value-based methodology. Ignoring these changes can have a profound effect on your cash flow and profitability.